| A | B |
|---|
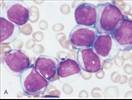
 | Precursor B cell: CD19, CD10, TdT |
| t(12;21) – CBFα /ETV6, t(9;22), t(4;11) |
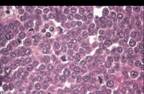
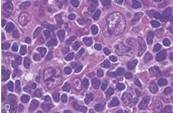
| lobulated nucleus, starry sky with tingible body macrophages |
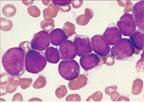
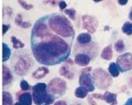
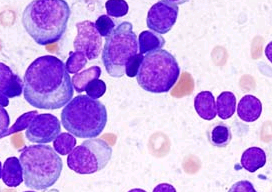
 | M0-M7 |
| CD 34, CD33, CD15 | |
| t(8;21) and inv(16) form CBF1α and CBFβ fusion protein, blocks terminal differentiation |
| acute promyelocytic leukemia: |
| Deletions in xsomes 5,7 following myelodysplastic syndromes or exposure to DNA-damaging chemo/radiation |
| Translocation of MLL gene on xsome 11q23 after topoisomerase II inhibitor treatment |
| Myeloblasts: delicate nuclear chromatin, 2-4 nucleoli,fine, azurophilic, peroxidaze + granules, red peroxidase + Auer rods |
| Monoblasts: folded or lobulated nuclei, no Auer rods, peroxidase - nonspec. esterase + | |
| Monocyte tumors in the skin and gingival, CNS spread |
| Good prognosis for t(8;21) or inv(16) w/ chemo | |
 | Cytotoxic CD8 T cell |
| Rearranged 2p23 with ALK gene | |
| Tumor cells cluster around venules and infiltrate lymphoid sinuses |
| Anaplastic Large Cell Lymphoma | |
 | Translocationof c-myc and Ig loci, t(8;14), t(8;22), t(2;8) |
| CD19, CD20, CD10, BCL6, IgM, κ or λ light chain-- LIKE DARK ZONE |
| EBV in endemic African cases, 15-20% of sporadic and 25% HIV | |
 | EBV in endemic African cases, 15-20% of sporadic and 25% HIV |
| AGGRESSIVE:Responds well to short-term, high dose chemo | |
| Jaw (mandible) or extranodal abdominal masses, |
 | Trisomy 12, deletions of 11q, 13q, 12q, 17p |
| Naïve B-cell or post germinal center memory B-cell | |
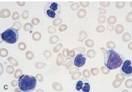
| CD19, CD 20, C23, CD5 |
| Prolymphocytic transf. to diffuse lg B-cell lymphoma (Richter syndrome) | |
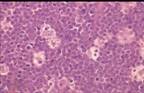
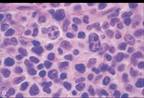
| Node: Larger prolymphocytes aggregate into mitotically active proliferation centers |
| Indolent, median sv.4-6 y, worse pronois w/ 11q 17p | 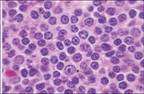 |
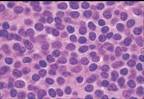
| Diffuse pattern of small lymphocytes peripheral blood may be leukopenic |
 | Diffuse Large B-Cell Lymphoma |
| BCL6 dysregulation on 3q27,t(14;18), cREl amplification | |
| Single rapidly growing mass, extranodal, common at Waldeyer ring, liver, spleen | |
| Immunodef.- associated (HIV, SCID, transplants, EBV) |
| Rapidly fatal if untreated; Chemo: 60-80% remission | |
| germinal or < center B cell CD19, CD20, TdT -; vrble exprssn of CD10, BCL6, SIg, |
| All ages (5% childhood lymphomas), most commonly adults (60 yrs), slight male predominance | |
 | Megakaryocytes have decrease requirement for growth factors |
| Hematopoietic stem cell that gives rise mainly to megakaryocytes | |
| Erythromelalgia – burning and throbbing in hands and feet caused by occlusion of small arterioles with platelet aggregates |
 | CD19, CD20, CD10, SIg, BCL2, BCL6 |
| t(14;18)-BCL2 and IgH - antiapoptotic |
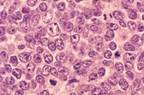
| Nodes:Centrocytes – small cleaved cells (majority) |
| most common form of NHL in the U.S. |
 | Centroblasts – larger, open chromatin, several nucleoli, modest cytoplasm |
| 30-50% transform to diffuse large B-cell lymphoma with survival |
| Follicular Lymphoma |
| Indolent, Incurable, median survival 7-9 years (good prognosis, low grade) |
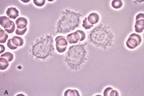 | CD19, CD20, IgG, κ or λ light chain, CD11c, CD25, CD103 |
| hairlike projections, round, oblong or reniform nuclei, moderate pale blue cytoplasm |
| Pancytopenia, |
| Post germinal center memory B cell |
| Older Caucasian males, Indolent, Sensitive to chemo |
 | Monoclonal,HLA-DR, S-100, CD1A, CCR6 and CCR7 |
| Abundant, vacuolated cytoplasm containing Birbeck granules (tennis-racket), vesicular nuclei with linear grooves or folds |
| Multifocal multisystemic: rapidly fatal if untreated, intensive chemo – 50% survive 5 yrs |
 | Secreted IgM for plasma cells |
| B-cells, plasma Cells, deletion on 6q; Older adults (60-70 yrs) |
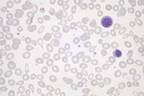
| Lymphoplasmacytic Lymphoma |
| Bone Marrow:Lymphocytes, plasma cells and intermediate plasmacytoid lymphocytes, hyperplasia of mast cells |
| PAS positive inclusions of Ig in cystoplasm (Russell bodies) or nucleus (Dutcher bodies) |
| IgM causes Hyperviscosity syndrome |
| Weakness, fatigue, weight loss, lymphadenopathy, hepatosplenomegaly, anemia (autoimmune hemolysis by cold agglutinins at <37 C) |
| (Waldenstrom macroglobulinemia) – visual impairment, headaches, dizziness, deafness, bleeding, cryoglobulinemia (precipitation of macroglobulins at low T) |
| Plasmapheresis alleviates hyperviscosity and hemolysis, incurable, progressive Meidan survival: 4 yrs |
| Transformation to large-cell lymphoma |
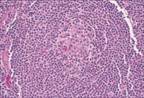
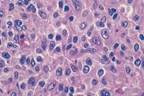
 | Mantle Cell Lymphoma |
| CD19, CD20, IgM, IgD, κ or λ light chain, CD5, Cyclin D |
| t(11;14) involving BCL1 (cyclin D1) and IgH |
| Node:Tumor cells surround reactive germinal centers |
| Disseminated disease, painless lymphadenopathy, bone marrow, splenic white pulp, hepatic periportal areas, gut, lymphomatoid polyposis |
 | Naïve B cell |
| Small lymphocytes with round or clefted nuclei, condensed chromatin, inconspicuous nucleoli, scant cytoplasm |
 | Myelodysplastic Syndromes: Pawn ball megakaryocytes (single nuclear lobes or multiple separate nuclei) |
 | Survival dependent on IL-6 produced by neoplastic plasma cells and normal stromal cells in the marrow |
| Neoplastic plasma cells produce osteoclast factors MIP1α and RANKL (R’ for NF-κB) |
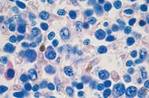
| Multiple Myeloma, Solitary Plasmacytoma, Monoclonal Gammopathy of Uncertain Significance (MGUS) |
 | Most common symptomatic monoclonal gammopathy |
| Chemo with alkylating agents 50-70% remission with survival of 3 yrs |
| Gelatinous soft, red tumor masses esp. in vertebral column, ribs, skull. |
| Osteoprotegrin inhibits RANKL, |
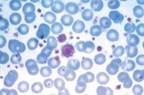
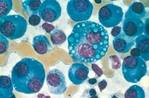
 | multiple myeloma Intracellular accumulation of degraded Ig – flame cells with red cytoplasm |
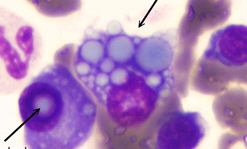 | (Russell bodies – cytoplasmic, Dutcher bodies – nuclear) Multiple myeloma |
blue grapelike cytoplasmic droplets, inclusions of fibrils, crystalline rods and globules, 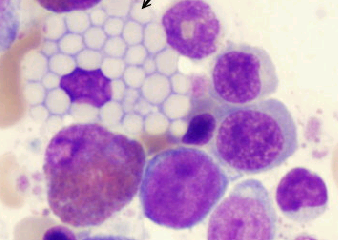 | multiple myeloma, Mott cells |
| Plasmacytosas and MGUS may progress to MM |
| Older adults (50-60 yrs), men, African descent |
| Plasma cells infiltrate marrow diffusely or in sheetlike masses. |
| Lytic bone lesions, pathologic fractures, renal failure (myeloma kidney), primary amyloidosis, hypercalcemia |
| Small Lymphocytic Lymphoma (Nodal) |
 | Nucleated Red Cell Progenitors |
 | CD2, CD5, CD3, αβ or γδ receptor, sometimes CD4, CD8 |
| Diffuse involvement of lymph node:Variable sized T cells, eosinophils, macrophages, angiogenesis |
| Peripheral T-Cell Lymphoma, Unspecified |
| Mature T cells: Diffuse involvement of lymph node |
| Lymphadenopathy, eosinophilia, pruritus, fever, weight loss |
| Worse than comparable B cell neoplasms; poor prognosis but some cures reported |
 | Multipotent myeloid stem cell that gives rise to erythrocytes, granulocytes, megakaryocytes |
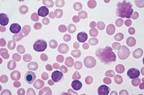
| Peripheral blood: basophilia, polycythemia, granulocytosis, thrombocytosis |
 | fibrosis in bone marrow specimen: often referred to as the spent phase of polycythemia vera |
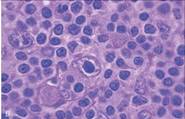
 | Lymphocyte predominance Reed Sternberg Cells |
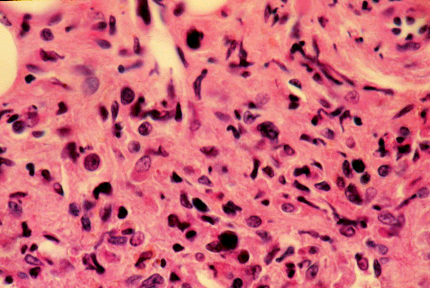
 | Primary Myelofibrosis: Identical to spent phase of other chronic myeloproliferative disorders |
| Rapid dev. of obliterative marrow fibrosis due to inappropriate release of PDGF and TGFβ from neoplastic megakaryocytes |
| Peripheral blood:dacryocytes (tear-drop erythrocytes), large platelets, basophilia, cytopenias, Leukoerythroblastosis-erythroid/granulocytic precursors |
 | Ringed sideroblasts- erythroblasts with iron laden mitochondria |
 | Pseudo-Pelger-Huet cells – PMNs w/ 2 nuclear lobes |
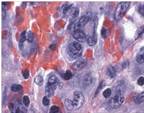
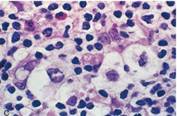
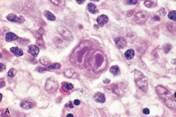 | Reed Sternberg Cell |
| Hodgkin Lymphoma |
| Giant RS cells that secrete IL-5, IL-6, IL-13, TNF, GM-CSF, attracting lymphocytes, macrophages and granulocytes which in turn support growth of the tumor cells |
| -During cell death cell shrinks and becomes pyknotic (mummification) |
 | Mediastinal mass in young females. Moderately aggressive. |
| Nodular sclerosis most common HL (65-70%) |
 | RS Mononuclear Variant; Single round or oblong nucleus; Large inclusion like nucleolus |
| R-S cells found in HL of Mixed cellularity,Lymphocyte-rich |
